Does lung cancer have its own tenants?
A supporting character in the drama

The presented study suggests that an aggressive tumor may sometimes create conditions conducive to the presence of an opportunistic fungus. This is another step toward an increasingly complex understanding of cancer—one that takes into account not only a collection of abnormal cells, but also their microenvironment.
For years, lung cancer has been described in language familiar to both patients and physicians—mutations, metastases, computed tomography, surgery, chemotherapy, immunotherapy. It is the vocabulary of a battle against one of the most serious diseases of our time. Yet alongside this traditional image, a second, more complex one is emerging. A tumor is no longer seen solely as a mass of cells that have escaped control. Increasingly, it is presented as a biological environment, with blood vessels, immune cells, inflammation, altered metabolism, and a network of local interactions.
Researchers are now attempting to add another element to this picture: microorganisms.
A new study by a team from the Wroclaw Medical University, published in Frontiers in Cellular and Infection Microbiology, addresses a question that would have sounded surprising just a few years ago—can lung cancer tissue serve as a site of colonization by Pneumocystis jirovecii, an opportunistic fungus known primarily for causing severe infections in immunocompromised individuals?
The wrocław study

The lead author of the study is Dr. Magdalena Szydłowicz from the Department of Biology and Medical Parasitology, Faculty of Medicine, Wroclaw Medical University. Together with collaborators from the 4th Military Clinical Hospital in Wrocław and scientists from the Czech Republic, Spain, and France, the team combined microbiological, clinical, and molecular expertise to determine whether Pneumocystis jirovecii DNA could be detected in tissue samples collected from patients undergoing lung cancer surgery.
“Our interest was not merely in detecting Pneumocystis, but in asking whether the tumor microenvironment promotes infection by this pathogen. At the same time, the reverse relationship is also possible—the presence of Pneumocystis, by inducing local inflammation or other changes in lung tissue, may potentially influence the course of neoplastic processes,” says Dr. Magdalena Szydłowicz.
This study belongs to the category of exploratory research. It does not test a new drug. It does not compare two treatment methods. It does not alter standards of care. Its aim is to determine whether a particular biological phenomenon exists at all and whether it is worth further investigation. In science, progress often begins with such questions.


From left: Żaneta Zajączkowska, PhD; Magdalena Szydłowicz, PhD; Marta Kicia, DSc, Associate Professor – Department and Division of Medical Biology and Parasitology, Wroclaw Medical University
From left: Żaneta Zajączkowska, PhD; Magdalena Szydłowicz, PhD; Marta Kicia, DSc, Associate Professor – Department and Division of Medical Biology and Parasitology, Wroclaw Medical University
What is Pneumocystis jirovecii?
It is a fungal species historically associated mainly with pneumonia in individuals with severe immune deficiencies—patients with AIDS, transplant recipients, or those undergoing intensive oncological treatment. In such cases, it can cause a severe disease requiring urgent treatment.
However, this is only part of the picture.
An increasing number of studies show that infection with Pneumocystis jirovecii may also occur without classical disease symptoms, in the form of colonization. In practice, this is like a situation in which someone is present in a building but causes no damage. They are there, but do not engage in open conflict.



Cancer as a habitat
A tumor does not grow in isolation. Cancer cells secrete chemical substances, influence blood vessels, alter local pH, and attract or repel immune cells. A specific microenvironment forms around the tumor. It is precisely this environment that now interests oncologists as much as the tumor itself.
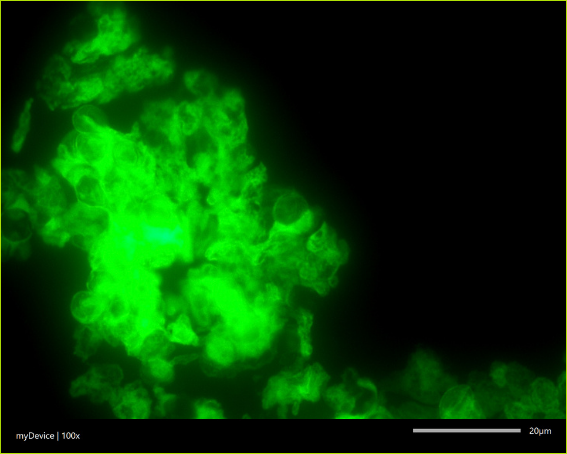
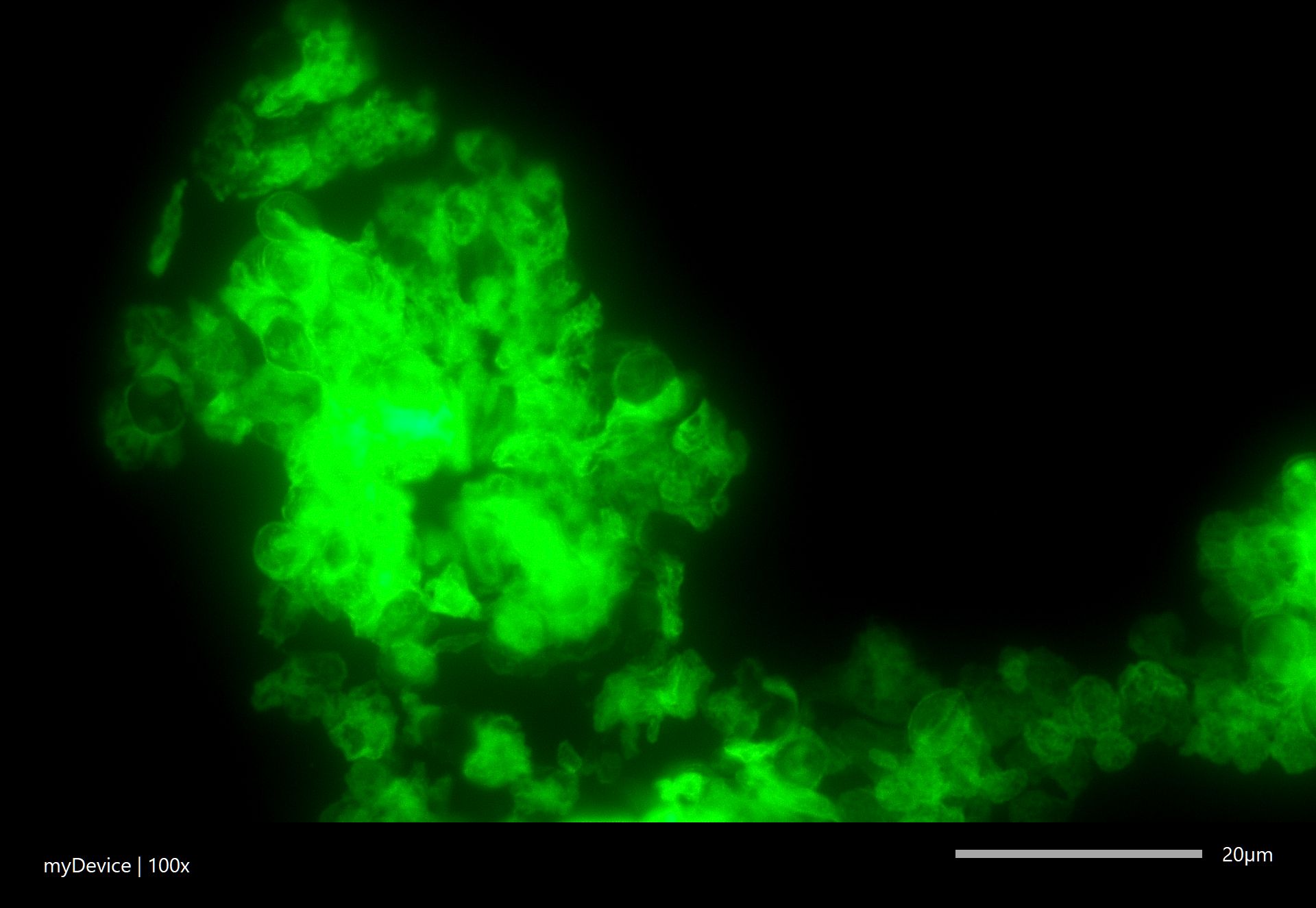
Cysts of Pneumocystis jirovecii in a sample collected from a patient with pneumocystosis, stained using the indirect immunofluorescence method.
Cysts of Pneumocystis jirovecii in a sample collected from a patient with pneumocystosis, stained using the indirect immunofluorescence method.
Because the course of disease is often determined not only by the mutations that led to cancer development, but also by the surrounding context. Is the immune system active? Is there chronic inflammation in the tissue? Does the tumor have good vascularization? Does it respond to immunotherapy?
To this list of questions, researchers from Wrocław have added another: which microorganisms may be present there?
Podcast:
Click here to listen!
The setting of the stage
The study included 70 patients with primary lung cancer, operated on between 2023 and 2025. Importantly, these were patients prior to chemotherapy and without recent immunosuppressive treatment. This was intended to limit the influence of therapy on the results.

During surgery, three types of material were collected: a fragment of tumor tissue, a fragment of adjacent lung tissue that appeared macroscopically unaffected, and secretions from the lower respiratory tract. Using PCR methods, researchers then searched for Pneumocystis jirovecii DNA in these samples. Molecular detection allows identification of the pathogen even at low infection intensity, characteristic of colonization.

A supporting character in the drama
Fungal DNA was detected in 8 of 70 patients (11%) in the study group. In some cases, genetic material was present in respiratory secretions or in adjacent lung tissue. Most notably, however, it was detected in tumor tissue from only two patients.
Both cases involved lung adenocarcinoma with a high degree of malignancy.
“In our observations, this fungus was detected in tumor tissue in patients with more advanced cancer, which may suggest that such an altered tumor environment promotes colonization by Pneumocystis. However, it must be emphasized that this is a preliminary observation and requires further research,” notes Dr. Szydłowicz.
This is an intriguing observation, but one that requires caution. Two cases are not sufficient for broad generalizations. They may, however, indicate a direction for further research. It is possible that more aggressive tumors create an environment more susceptible to colonization by certain microorganisms.


What the study does not show
In an era of rapid headlines, it is important to state clearly: the study does not show that the fungus causes lung cancer. It does not suggest that cancer patients should receive antifungal prophylaxis. Nor does it prove that the presence of Pneumocystis worsens prognosis.
It merely shows that in some patients, genetic material of this organism can be detected, and in rare cases, also within tumor tissue.
So why does this matter?
Modern medicine often advances through such incremental shifts in knowledge. First, a signal appears. Then, other teams verify it in larger patient groups. Only after years does it become clear whether it was a valid lead.
Today, similar questions are already being asked across many fields of oncology. It is known that the bacterium Helicobacter pylori increases the risk of stomach cancer. The HPV virus plays a significant role in cervical cancer. In colorectal cancer, the role of specific gut bacteria is under investigation. Increasingly, the impact of the gut microbiome on the effectiveness of immunotherapy is also being analyzed.
The patient is on stage
A patient with lung cancer should not, based on this study, request testing for Pneumocystis. A physician will not change therapy based on reading a single scientific article. No new clinical recommendations emerge from this work. Its significance lies elsewhere—it illustrates how our understanding of cancer is evolving.
Not long ago, cancer was described almost exclusively as a genetic problem. Then it also became an immunological problem. Today, it is increasingly viewed as a complex condition, dependent on interactions among cancer cells, the immune system, inflammation, and microorganisms.
This will not change the treatment tomorrow morning. But it may change treatment in the years to come.
The authors themselves emphasize the study’s limitations. The patient group was small, and only two positive results were found in tumor tissue. This is insufficient for drawing strong conclusions.
Larger-scale studies, ideally multicenter, are needed to determine whether this observation is reproducible in other populations. It will also be important to determine whether the pathogen's presence affects inflammation, treatment response, or prognosis.
“For now, we are at the stage of observation, not clinical practice. However, our results may provide a foundation for future studies on the role of the lung myco- and microbiome in the context of tumor immunology, as well as potential diagnostic and prognostic biomarkers,” adds Dr. Szydłowicz.


Science slowly reveals the stage
The work of Dr. Magdalena Szydłowicz’s team is precisely such a building block. Not a breakthrough, not a sensation, not a promise of a new therapy. Rather, a carefully posed question and a first attempt at an answer. In science, that is a great deal. Before treatment emerges, a better understanding must come first. And it almost always begins with someone daring to look where few have looked before.
D. Sikora
FAQ
1. What was the main objective of the study?
The main objective was to determine whether the opportunistic fungus Pneumocystis jirovecii can colonize lung tumor tissue, and whether it accumulates directly within the tumor.
2. What patient group was analyzed?
The study included 70 patients with histologically confirmed primary lung cancer who had not received chemotherapy or immunosuppressive treatment within six months prior to the study. Over 91% of cases were non-small cell lung cancers (NSCLC).
3. What types of samples were collected?
Three types of material were collected intraoperatively: tumor tissue (NPL), adjacent non-tumorous tissue (NAT), and respiratory secretions (RS).
4. How often was P. jirovecii detected?
Fungal DNA was detected in 8 of 70 patients (11.4%) across 14 samples.
5. Was the pathogen found in tumor tissue?
Yes, P. jirovecii DNA was detected in tumor tissue in two patients. In both cases, it was present in all three sample types (NPL, NAT, RS).
6. Is there a link between tumor grade and fungal presence?
Yes. The presence of Pneumocystis in tumor tissue was observed only in patients with high-grade (G3) tumors, suggesting that advanced cancer may create a microenvironment favorable to colonization.
7. What laboratory methods were used?
Nested PCR targeting mitochondrial genes (mtLSU rRNA and CYB) was performed, followed by SNP-based genotyping.
8. Did patients show symptoms of pneumonia?
No. None had clinical or radiological signs of pneumocystis pneumonia (PCP); they were classified as colonized.
9. Why is colonization clinically relevant?
Even in the absence of symptoms, colonization may induce inflammation and tissue damage. In cancer patients, it may increase the risk of developing full-blown PCP, especially during immunosuppressive treatment.
10. What are the key clinical implications?
The authors suggest considering screening in this patient group before oncological treatment and highlight the potential role of the lung microbiome as a diagnostic and prognostic biomarker.
Powerd by NotebookLM

This material is based on the article:
Multi-site screening for Pneumocystis jirovecii in lung cancer: possible tumour tissue colonization
DOI: 10.3389/fcimb.2026.1755638
Authors: Magdalena Szydłowicz, Żaneta Zajączkowska, Mariusz Chabowski, Maciej Nowicki, Błażej Łukianowski, Paweł Gajdzis, Martin Kváč, Enrique J. Calderón, Solène Le Gal, Marta Kicia
Web. A. Maj
Photos: freepik.com